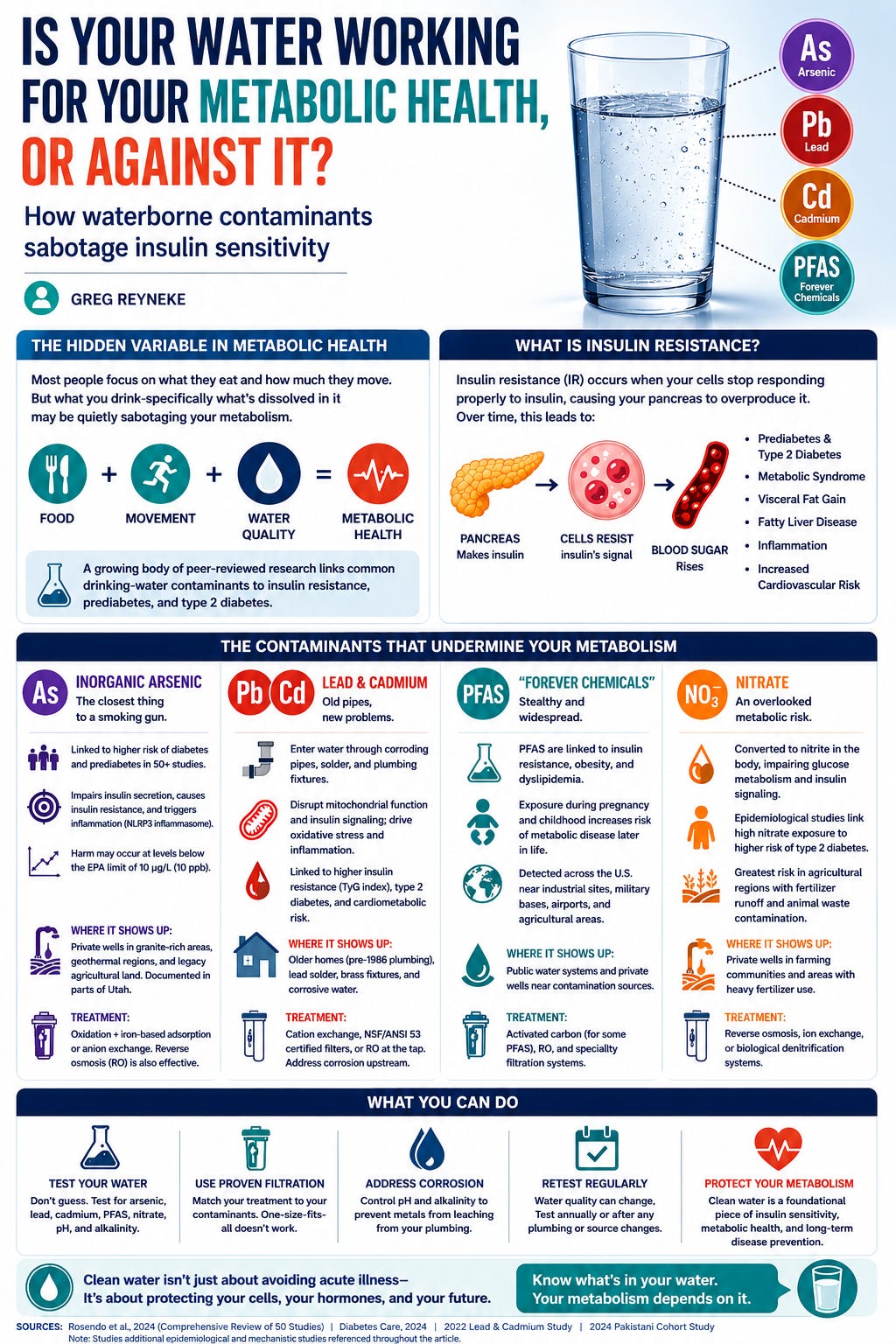
Most people think about insulin resistance in terms of what they eat and how much they move. Those things matter enormously, but there’s a third variable almost nobody talks about: what they drink, and specifically, what’s dissolved in it.
There is a growing body of peer-reviewed evidence linking common drinking-water contaminants to insulin resistance, prediabetes, and type 2 diabetes. This isn’t fringe science, these findings come from meta-analyses, longitudinal cohort studies, and mechanistic research published in journals like JAMA, Diabetes Care, and Molecular Metabolism.
Let me walk you through what the science actually says, and what you can do about it.
What Is Insulin Resistance, and Why Does It Matter?
Insulin resistance (IR) is the condition where your cells stop responding properly to insulin, the hormone your pancreas secretes to move glucose out of your bloodstream and into your tissues. When cells resist insulin’s signal, your pancreas compensates by producing more. Eventually, the system breaks down: blood sugar rises, fat metabolism shifts, inflammation increases, and the cascade toward prediabetes and type 2 diabetes begins.
IR is also the engine behind metabolic syndrome, visceral fat accumulation, non-alcoholic fatty liver disease, and a significant portion of cardiovascular risk. Diet and physical activity are the primary levers. But if your water supply is chronically loading you with metabolic disruptors, you’re effectively fighting that battle with one hand tied behind your back.
Contaminants That Undermine Your Metabolism
Inorganic Arsenic: The Closest Thing to a Smoking Gun
Arsenic in groundwater is the most extensively studied waterborne metabolic disruptor, and the evidence is damning.
A comprehensive review of 50 studies found that arsenic exposure was consistently associated with increased risk of diabetes and prediabetes in humans, along with measurable impacts on blood glucose and insulin resistance in both human and animal models (Rosendo et al., 2024). A 2024 study was published in Diabetes Care, examining data from the Multi-Ethnic Study of Atherosclerosis and the Strong Heart Study. It directly linked water arsenic exposure to incident type 2 diabetes in U.S. adults, including people drawing from regulated community water systems, not just private wells.
Mechanistically, the picture is clear. Chronic arsenic exposure impairs insulin secretion from pancreatic beta cells, induces glucose intolerance, and promotes insulin resistance through oxidative stress, disruption of PI3K/Akt signaling pathways, and NLRP3 inflammasome activation. In animal studies, arsenic exposure even at sub-toxic concentrations, levels designed to simulate real-world chronic exposure) produced elevated blood glucose and measurable beta-cell dysfunction.
Here’s the part that should concern anyone on a well or in a high-arsenic region: the EPA’s maximum contaminant level (MCL) for arsenic is 10 µg/L (10 ppb). Epidemiological data suggest metabolic harm may occur at exposures well below that regulatory threshold with long-term chronic exposure. Meeting the legal standard doesn’t necessarily mean you’re in the clear biologically.
Where arsenic shows up: Private wells drawing from granite-rich aquifers, geothermal areas, and legacy agricultural land. In Utah, arsenic is a documented issue in multiple counties (Particularly in Utah County and proximal areas). It’s also present in some municipal supplies at levels below the MCL that are still concerning over time.
Treatment: Oxidation to convert As(III) to As(V), followed by iron-based adsorption media or strong-base anion exchange. Reverse osmosis is also effective but requires proper pretreatment to prevent membrane fouling.
Lead and Cadmium: Old pipes, new problems
Lead and cadmium enter drinking water through corroding pipes, solder joints, and plumbing fixtures, not just the source water. A 2022 study found co-exposure to lead and cadmium significantly associated with type 2 diabetes and obesity in community populations. Higher blood levels of both metals correlate with elevated TyG index (a validated surrogate marker for insulin resistance) and increased cardiometabolic risk.
The mechanism: cadmium disrupts mitochondrial function and induces oxidative stress in liver, muscle, and adipose tissue; the same tissues that govern insulin sensitivity. Lead compounds this by impairing the insulin signaling cascade directly. The result is a combination of hepatic insulin resistance and hyperinsulinemia that looks disturbingly similar to diet-induced metabolic syndrome.
A 2024 Pakistani cohort study of diabetics found that elevated groundwater lead above WHO limits correlated with higher fasting glucose, HbA1c, dyslipidemia, and inflammatory markers after controlling for other variables.
Where this shows up: Older homes (pre-1986 plumbing), buildings with lead solder, brass fixtures leaching into soft or acidic water. This is not hypothetical. The Flint crisis was an extreme case, but low-level lead leaching from in-home plumbing is widespread and largely invisible without testing.
Treatment: Cation exchange, certified point-of-use filtration (NSF/ANSI Standard 53), or RO at the tap. Critically: if your source water is corrosive (low pH, low alkalinity), you need corrosion control upstream; treating at the tap without addressing corrosion is incomplete.
The “Forever Chemicals” can also be metabolic disruptors
Per- and polyfluoroalkyl substances (PFAS) contaminate drinking water supplies across the Unites States. Elevated levels have been concisely found near military bases, industrial sites, airports, and agricultural areas where PFAS-containing firefighting foam was used. They’re hyperbolically called “forever chemicals” because their carbon-fluorine bonds resist degradation both in the environment and in the human body; some PFAS compounds can persist for years before breaking down. Not all PFAS are the same and the risks vary based on their molecular size.
The metabolic evidence is building. A July 2025 study published in eBioMedicine(Mount Sinai School of Medicine) found that higher blood PFAS levels were associated with a 31% increased risk of developing type 2 diabetes with each step up in exposure quartile (in a diverse U.S. population of regular New Yorkers, not just people with unusual occupational exposure). A Swedish register-based study of over 55,000 adults found an increased risk of type 2 diabetes, including earlier-onset disease, in people with long-term high PFAS exposure through drinking water.
Mechanistically, PFAS appear to disrupt glucose homeostasis through amino acid metabolism dysregulation, cytochrome P450 pathway interference, and direct disruption of insulin secretion from beta cells via GPR40 receptor activation. In animal models, PFAS exposure consistently produces hyperglycemia and impaired glucose tolerance.
The caveat: epidemiological evidence on PFAS and T2D is not yet as consistent as the arsenic literature. Some studies show neutral or inverse associations depending on specific compounds and exposure levels. But the direction of evidence, the mechanistic plausibility, and the July 2025 human data all point in one direction: this is a real concern, not a speculative one.
Where PFAS shows up: Groundwater and surface water near military installations, airports, industrial manufacturers, and certain agricultural regions. PFAS contamination is often invisible, with no taste, odor, or color. You will not know PFAS are there without testing.
Treatment: Activated carbon (AC) in granular or block format, specialty Anion Exchange (IX), and high-rejection reverse osmosis are currently the three proven approaches. IX and AC are effective but require proper sizing and media replacement discipline as well as consideration of contact times. PFAS will of course break through a saturated AC or IX bed, so maintenance is key. RO provides reliable broad-spectrum removal, but the concentrate waste stream is just “kicking the can down the road” to be dealt with later…
Magnesium in water can be helpful
Not everything dissolved in water hurts you. Magnesium is a critical cofactor in insulin signaling. It is required for GLUT4 translocation (the mechanism that moves glucose into cells), for insulin receptor function, and for glucose metabolism at the cellular level.
The research is consistent: magnesium deficiency is associated with insulin resistance, and restoring magnesium sufficiency measurably improves insulin sensitivity. A 2023 randomized controlled trial published in npj Clean Water found that adding magnesium to desalinated drinking water significantly improved fasting insulin, HOMA-IR (a validated measure of insulin resistance), and lipid profiles in patients with type 2 diabetes. A 2024 randomized trial confirmed that magnesium-enriched deep-sea water markedly improved insulin sensitivity in prediabetic patients across multiple validated metrics. A meta-analysis of 23 randomized controlled trials found that magnesium supplementation significantly reduced fasting blood glucose in diabetic patients.
Beneficial treatment technologies like softening and reverse osmosis both strip magnesium from water (if it was ever there to start with). Treated water that is very low in mineral content (especially post-RO water) may potentially be contributing to chronic low-grade magnesium deficiency if dietary magnesium intake is also marginal (which it frequently is in Western diets).
Post-treatment remineralization (using alkalinity enhancement cartridges, blended mineral injectors, cartridges, or controlled dosing is an evidence-based step toward mineral-balanced water that works for your metabolic health while also actively protecting plumbing infrastructure. Naturally, the amount of beneficial minerals consumed from drinking water lone is not sufficient to preserve or promote good health; this all assumes that one is eating a healthy diet
What this means practically
The regulatory system is designed to protect against acute toxicity and known carcinogens. It is not optimized around chronic low-dose metabolic disruption from contaminant mixtures. Hitting the MCL for arsenic doesn’t mean chronic exposure is metabolically harmless. Municipal water compliance reporting tells you what was tested, not everything that could be in the water, or that potentially has an impact.
The honest position is this: you cannot assume your water is metabolically neutral without data. You need to know what’s actually in it.
Three things you can do right now
Step 1: Get your water tested. This is not optional if you’re serious about metabolic health. A basic water quality panel from a certified laboratory will cover arsenic, lead, cadmium, hardness, pH, TDS, and bacteria. If you’re on a well in a high-arsenic region (Utah, the Southwest, New England, Midwest agricultural areas), arsenic testing is non-negotiable. PFAS testing is more expensive but warranted if you’re near a known contamination source. Your local health department can often direct you to a certified lab. Start with data, not assumptions.
Step 2: Have a qualified water treatment professional evaluate your results. A water test report is raw data. The interpretation (what treatment is appropriate, what media works for your specific contaminant profile, what post-treatment remineralization is needed) requires engineering judgment. A licensed, credentialed water treatment professional (look for WQA Master Water Specialist certification) will design a system to your specific source water, not just sell you a generic product. Beware of any company that recommends a solution before they’ve evaluated your water chemistry.
Step 3: Address the mineral balance of your treated water. If you’re running a whole-house RO or an aggressive softening system, talk to your water treatment provider about post-treatment remineralization. This isn’t complicated — it’s a well-understood engineering step — but it’s often skipped. Magnesium-balanced water costs almost nothing extra to produce and has a clear evidence base behind it.
The bottom line
Your water supply is either supporting your metabolic health or quietly undermining it. Arsenic impairs beta-cell function and insulin sensitivity at levels that are within EPA’s SDWA standards. Lead and cadmium drive oxidative stress and hepatic insulin resistance. PFAS disrupt glucose homeostasis and are now linked to a 31% increase in T2D risk in human populations. And purified, low-mineral water may possibly be contributing to the magnesium deficiency that makes insulin resistance worse.
None of this replaces diet, exercise, sleep, or medical care. But it’s a variable you have the ability to control, and most people never even look at it.
Get your water tested, know what you’re drinking, and take control of one more lever towards improving your health and happiness.
https://gregreyneke.substack.com/p/is-your-water-working-for-your-metabolic